As part of our daily life we are exposed to many different types of risks. This document is a thorough risk assessment tool of a client. This document assesses the risk to a client in all aspects of a client’s life and identifies strategies and supports to minimise the risks. The plan may reference other documents such as Behaviour management plans, mealtime management plans, etc.
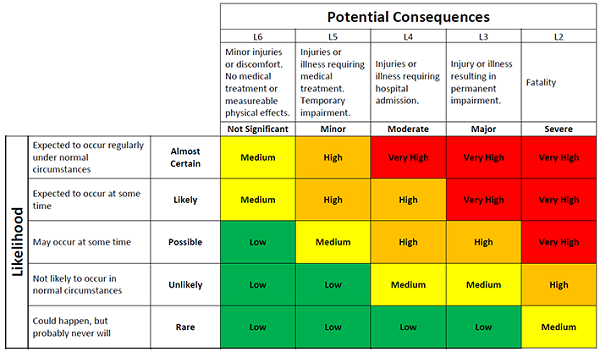
This plan identifies the level of risk to a client and to others, of each identified risk and then identifies the risk again with the strategies for reducing the risk in place.
This plan is a very important document for a carer to be familiar with as this document will outline all the potential risks to the client and their level of understanding of the risks. It outlines strategies to manage that risk and refers you to other documentation to further support the carer in understanding how to manage a particular risk.
As part of our daily life we are exposed to many different types of risks. This document is a thorough risk assessment tool of a client. This document assesses the risk to a client in all aspects of a client’s life and identifies strategies and supports to minimise the risks. The plan may reference other documents such as Behaviour management plans, mealtime management plans, etc.
This plan identifies the level of risk to a client and to others, of each identified risk and then identifies the risk again with the strategies for reducing the risk in place.
This plan is a very important document for a carer to be familiar with as this document will outline all the potential risks to the client and their level of understanding of the risks. It outlines strategies to manage that risk and refers you to other documentation to further support the carer in understanding how to manage a particular risk.
In the event of a medical emergency a client’s care plans and case management form an excellent resource for medical staff to treat a client. The care plans outline what care a client is currently receiving and a client’s medical history.
Contains Clients Intervention History
Plans document what treatments have been implemented for a client both their current interventions as well as past interventions. This assists medical and other specialists in determining a treatment plan for the client. It informs them on what worked for the client previously and what has not worked.
Enables Specialist Collaboration
By having the client’s care requirements documented it also provides the information to medical and other specialists on the other treatments a client may be receiving from another specialist. This means that all specialists are working collaboratively to provide the best quality of care for the client.
Helps with NDIS Claim
The care plans and data collection process are an excellent source of information that can be provided as supporting evidence for a claim under a client’s NDIS Plan.
Help Care Staff
It outlines the client’s current care requirements. It informs care staff on what conditions the client has and how they need to manage the client’s care.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok












{kind=link}